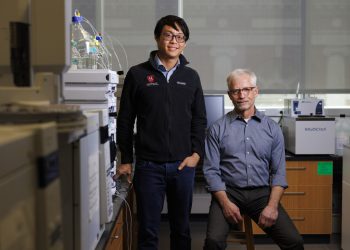

Stephanie Mitchell/Harvard Staff Photographer
Health
‘This is it. This is exactly what I want to do.’
Michael VanRooyen started running toward trouble more than 30 years ago. He’s still going.
Part of the
Experience
series
Scholars at Harvard tell their stories in the Experience series.
Michael VanRooyen has spent decades responding to emergencies around the world, with no choice but to stare straight ahead at suffering, destruction, and death. These experiences have taught him how to ease pain amid chaos, forced him to navigate moments of intense fear and danger, and given him the technical and emotional depth to support war-torn communities in their efforts to heal and rebuild.
“It’s a gift to work in a place where you truly feel like you are helping people,” he says. “I have always thought of it that way.”
VanRooyen, an emergency room doctor by his earliest training, is the J. Stephen Bohan Professor of Emergency Medicine at Harvard Medical School and the Lavine Family Professor of Humanitarian Studies at the Harvard T.H. Chan School of Public Health. In 2005, he helped found the Harvard Humanitarian Initiative, which in the years since has sought to strengthen aid programs through education and research. In this edited conversation, he reflects on the challenges and rewards of a calling that has taken him from big-city U.S. hospitals to global disaster zones and back again.
Where did you grow up?
A small town in Michigan called St. John’s, about 7,000 people. There were four of us — my father, my mother, my older brother Rick, and me. My parents grew up in Holland during World War II. As a young man, my father joined the Dutch resistance during the German occupation of the Netherlands in 1940. He was captured and imprisoned in Bergen-Belsen, a Nazi concentration camp. He was liberated at the end of the war and he and my mom immigrated to the U.S. in 1954. I remember being a little kid and wrapping my arm around his in church and asking about the numbers tattooed on his arm.
When I was 5, my mom was diagnosed with melanoma; she passed away on my eighth birthday. Three years later, my father married a woman with eight children, and suddenly I had five new sisters and three new brothers. It was quite an adjustment to suddenly be part of this big family, but it was great. My father was a cobbler and had his own shoe store, so we grew up with very limited means, but the family was close and very supportive. To get out of the house, I joined the Boy Scouts. When I was 14, I was with my scoutmaster when we witnessed a tractor crash. We called the paramedics and watched them in action. I was so impressed. I thought, “I have to do something like that.”
Tell me more about that crash.
My scoutmaster and I were driving along a country road when we came across a kid whose tractor flipped while trying to pull another tractor out of a ditch. He was pinned underneath the tractor, folded in half underneath thousands of pounds of metal. We were first on the scene. I was shocked and initially paralyzed. But he was alive, so my scoutmaster ran to a nearby house to call the paramedics while I held his hand and told him he would be all right. He was trapped and shaking, and we were both so scared. The paramedics arrived with a tow truck, and they started lifting the tractor. Everyone was so calm and professional during the rescue. They extricated him, loaded him in the ambulance, and got him to the hospital.
VanRooyen (second from left) as a youth with step-siblings (from left) Rose, Bill, and Joyce.
Photo courtesy of Michael VanRooyen
You were pre-med at Michigan State and then Wayne State for medical school. What do you remember most from those years?
I had a great experience at Michigan State, but pre-med was intense — physics, calculus, organic chemistry. It was a busy time — trying to work while going to school — but it prepared me well for medical school.
Wayne State Medical School was a bit of a culture shock. As a small-town kid, the urban environment of Detroit was an adjustment. But Detroit was an amazing place for clinical medicine because of the size and complexity of big hospitals like Detroit Receiving and Henry Ford Hospital. It was my first real exposure to emergency medicine. When I did my first rotation in the ER at Detroit Receiving Hospital — a massive department compared to anything I had experienced — there were sick patients everywhere. I watched the ER doctors and, just like the first responders I witnessed when I was a kid, they were all so professional and composed. The crazier it got, the more focused they became. On my first day in the ER, I thought, “This is it. This is exactly what I want to do.”
Are there any patients you still remember?
In the ER in Detroit, everything came through the door. I remember one patient who was working in the Chrysler plant and a container of molten plastic had spilled on him and hardened. A large part of his body, including his face and neck, was covered in black plastic. He could only breathe out of his nose, and we didn’t know how badly injured he was. We had to chip away all this plastic — there was an incredible mess in the emergency room. He was badly burned but alive underneath. We talked him through the procedure and got him to the ICU.
When did humanitarian response come into the picture?
I was a third-year student, bleary-eyed at 3 in the morning with a new admission. I was sitting next to the patient, asking him questions, when we both realized that we were falling asleep on the spot. We laughed about it and finished, but I remember walking out, looking out the window over the city and wondering what I wanted to do with my career. I was drawn to medicine to help people on their worst day and I wondered if it was possible to help people on a much larger scale. I imagined what my father went through as a war prisoner and wondered what it would take to work in the hardest places with the greatest need. I eventually decided to be a humanitarian doctor. I had no mentors and no experience. I had a lot of exploring to do, so I took three months off in my fourth year of medical school to work in El Salvador during the civil war. I returned to the U.S. with a new conviction to be a global doctor. I had found my calling.
After a magnitude 7.0 earthquake devastated Haiti in 2010, the Harvard Humanitarian Initiative, headed by VanRooyen (far left), mobilized to set up a field hospital.
Harvard file photo
Where was your residency?
University of Illinois in Chicago. I moved to Chicago, became an intern, and then did my residency in emergency medicine. Back then, there was no flexibility for travel abroad, so I went straight through residency — intense, but great — and graduated in 1991, a newly minted emergency physician. After working a year to pay off my student loans, I quit and headed abroad to explore global medicine. I spent the next year working in various international settings and eventually landed a position as a humanitarian doctor in Somalia. It was a sentinel moment for my career.
This was during the country’s civil war. What do you remember?
Rival clans fought for territory and the country was pushed into famine. Food relief shipments were being stolen by militias and sold for weapons. It was a very dangerous time for humanitarian organizations, which were trying to access the interior of the country to deliver food aid. Nongovernmental organizations had to adapt to the militarized context by paying for armed protection, so there were militias and weapons everywhere. I worked in Somalia over the course of 1992 and ’93, supporting medical care for refugees. Shortly thereafter, I was called to work in Bosnia in the former Yugoslavia to work in a war hospital. From there, I joined NGOs in a series of relief missions, managing teams in Rwanda after the genocide, then Sudan and other crises. I spent much of the 1990s back and forth between the U.S. and several humanitarian emergencies.
Were you an ER doctor doing humanitarian work on the side or the other way around?
Working in humanitarian crises and returning home to work in emergency medicine led to a set of parallel careers. Although the environments were completely different, I was able to leverage my experience from one with the other. I was a full-time emergency doc and director of an ER in Chicago at the same time as I was a relief doc with humanitarian organizations. I continued to grow my experience base, working with relief organizations in Bosnia, Kosovo, Iraq, and North Korea. Then I’d come home and resume my life as an ER doctor and professor. In 1997, I moved from Chicago to Baltimore to join the faculty at Johns Hopkins.
I want to backtrack to Rwanda. You worked in a refugee camp and then on restarting the Central Hospital of Kigali. Was that a different sort of project? It seems like a longer-term challenge.
The humanitarian relief work in Rwanda was massive and was largely setting up temporary facilities and healthcare — food, water, sanitation, housing — in these large camps. I originally went to a camp in Ngara, Tanzania, where there were over 400,000 refugees — it was incredibly challenging. But shortly thereafter, we followed the Tutsi military as they took back the country and came into Kigali. We arrived to find the hospital destroyed, with thousands of dead bodies, blood thick on the floor. It was a shocking site. Our job was to get the hospital up and running, starting with the operating rooms, emergency rooms, and some inpatient beds.
VanRooyen has cared for patients in war-torn areas such as Sudan, Iraq, and Bosnia.
Photos courtesy of Michael VanRooyen
Did you ever feel physically threatened in a danger zone?
There were times when it was logistically very difficult to get access to conflicted areas. Every trip had its challenges, and I got better at negotiating my way in, and knowing when to push harder and when to back down. It was common to get hassled at the border, made to negotiate with armed groups at a checkpoint. So any heightened sensitivity gets normalized after a while. Most of the time you learned to manage tense situations, but there were a few times when I felt truly threatened.
One of those times was in Zaire — now the Democratic Republic of the Congo — where I was working on a relief mission for refugees fleeing Rwanda. The minute we landed, we were accused of being spies. We were separated, interrogated at gunpoint, and then held for three days under house arrest. It was a highly volatile moment. Finally, with the help of two Zairian surgeons and about $6,000 that I had hid in my boots, we were deported. We hid in the back of a truck and made it to our plane and flew to Uganda. It was a harrowing experience.
Another episode happened when I was in Bosnia. We were crossing through Serb territory at night, trying to get into Sarajevo. In front of us, several Serb soldiers had pulled over a car, kicked out the windows, and dragged the driver out. They ran to us with their guns pointed at us and we just froze. We didn’t have our translator, so we put up our hands and yelled stuff like “From America … and New York … and Disneyworld!” They were finally amused — or disgusted — and shook their heads and let us go. Those are scary moments, which, fortunately, have been infrequent.
There are moments of fear, chaos, doubt in your work. Are there moments of joy and peace and satisfaction as well?
Overwhelmingly so. It’s a hard environment. There is a sense of guilt that comes from working amid such hardship and still having the ability to go back home. But it’s also an amazing opportunity to contribute and truly help people at the worst moment of their lives. It’s what I dreamed about all those years before in medical school. It’s a gift to work in a place where you truly feel like you are helping people. I have always thought of it that way.
When you’re training tomorrow’s humanitarian workers, how do you prepare them for things going wrong?
One of the reasons I started the humanitarian simulation training program 20 years ago was because of the gap between the classroom and what happens in the field. In the classroom, we would teach future humanitarian aid workers on issues of humanitarian principles and access and negotiation, but these concepts lacked the reality that aid workers face in the field. It’s hard for anybody sitting in class to think, “Am I really going to be at a roadblock and have to negotiate access with a gun in my mouth?” The simulation provides practical training. I wanted to give them the feeling of stress, and to help them understand the reality of what working in a conflict zone looks like. It has become the premier civilian humanitarian simulation in the world.
You were at Hopkins for seven years before moving to Harvard. How did one lead to the other?
I co-directed a humanitarian center at Johns Hopkins, developing the idea of bridging academics with humanitarian practice. While building the center, I worked as an emergency physician and continued to write and teach. Hopkins was a rich environment for both humanitarian studies and emergency medicine, and I grew a lot while I was there. I learned to work with U.N. agencies and major NGOs.
I was recruited to join the faculty at Brigham and Women’s Hospital and to launch a humanitarian program at Harvard. So, I partnered with Jennifer Leaning, a close colleague at Harvard, and essentially started all over again. On the flight to Harvard, I made one slide. It was called the “Harvard Humanitarian Institute.” That was the thing I wanted to build. With Jennifer, we created the concept of building a humanitarian university at Harvard. I believed that humanitarian assistance is not just medicine and public health; it is politics, law, economics, sociology, anthropology — nearly every discipline. And there’s no place like Harvard. We have programs, scholars, and students in just about every academic area, and I wanted to leverage the whole ecosystem to create this new center.
“I was drawn to medicine to help people on their worst day and I wondered if it was possible to help people on a much larger scale.”
Stephanie Mitchell/Harvard Staff Photographer
The initiative’s goal was to conduct research and develop tools that improved humanitarian work, addressing problems you saw in the field. What was wrong with humanitarian aid?
When I worked in Somalia, I realized that good intentions are not enough. Most people showing up to work in a highly pressured humanitarian setting had little experience and no training. As a Western emergency medicine doctor, I was entirely unprepared to work in a war zone. I didn’t know the culture, I didn’t know the context, I didn’t know a lot of the conditions I was treating. I was not prepared, and I was pretty sure most other people were also not prepared. It was a feature of the rapid growth of the aid industry. More conflicts, more crises, and more civilian aid agencies, with more people arriving without experience or training. It occurred to me that there was no professional pathway to train humanitarians. I felt like the humanitarian system needed a connection to research and education and a professional pathway for leadership development and mentoring, similar to what we have in medicine. The vision was that HHI would be among the very first organizations that aimed to professionalize the aid community at a time when it was growing rapidly and getting more dangerous.
How long before you decided that as an enterprise, aid efforts weren’t working?
First time.
Really?
Yes. When I worked in Somalia, I deeply admired the humanitarians I saw there. It was such important, lifesaving work in one of the most dangerous and complex places on earth. It was crucial work, and there were many dedicated, well-intentioned people trying to do good things, but failing at it. But the system was not built for learning. It didn’t encourage analysis or self-reflection, and there were few paths for professional development. The humanitarian system needed to evolve.
You once said that leadership is one of the hardest things to teach. Why is that the case?
If an instructor has never experienced the challenges of the field, I think it’s difficult to convey that in the classroom. In humanitarian studies, for example, my courses are derived from lessons in the field. Being a humanitarian in the field and bringing it back home to teach humanitarian studies gives it a level of validity that is different than if you just read the book. Leadership is the same in my opinion. Yes, you can teach leadership and theory, but if you haven’t faced the personal challenges of being a leader under challenging circumstances, it’s hard to teach that. Most leaders are not teachers, and most teachers have not been leaders. So having been fortunate to lead in emergency medicine, as a chair and as a systems leader, and also to have led in the humanitarian sector, I really draw from all of that to be able to develop this concept of who you are as a leader, because I’ve been there.
Is leadership intrinsic — are some people natural leaders — or can it be taught?
I don’t think leaders are necessarily born, though there are personality traits that make you better: a natural communicator, a unique sense of empathy, being good at self-editing on the fly. Those are not easy traits to gather into one person and some people will never get some of those right. But I do think that leadership, as a discipline, can be taught as a series of ideas, techniques, and practices.
Self-editing and empathy probably aren’t the first things that a lot of people would mention when they talk about good leaders. What about organization, persuasion, the arm-twisting that happens in politics?
Much of my daily function as a leader has to do with personal relationships: building capital for times when I have to make tough decisions. Another important skill is understanding and predicting problems, which are almost always people problems. I have worked with many gifted leaders, and watched them manage change, communicate in a crisis, or negotiate a difficult relationship. But what I’ve admired the most is the ability to be thoughtful, humble, self-reflective, and empathetic communicators who can express that they care. I think good leaders can blend the techniques of leadership while building strong relationships.
Is the humanitarian field better today?
The humanitarian sector has grown and advanced in its complexity, its use of evidence, and its impact. The sector has grown to meet the needs of hundreds of millions and is a lifeline for people around the world. But the humanitarian sector is facing its own crisis. The elimination of USAID and its mandate sent shock waves across the humanitarian world, forcing many organizations to radically downsize. It has also created a narrative that the vital humanitarian work that we do is somehow less important. Many NGOs and U.N. agencies have had to reduce their efforts. As the humanitarian sector adapts, there will be many unmet needs. HHI has to rethink our next steps in the field and see how we are going to contribute to the future of global aid.
In addition to your HHI work, you’ve led emergency care at the Brigham and you’re now chief of emergency medicine for Mass General Brigham. Take me through that role.
I’m the chief of the MGB system, so now I lead the MGH and BWH and our eight other emergency departments. Before MGB, we were a loose federation of individual emergency departments that operated quite independently. Pulling them all together into one MGB system was complex, but it is gratifying to see them come together and work as a team.
I think it’s important as a leader to stay clinically active, so I work once a week in the ED at MGH. We see everything, all day, every day. My work in the humanitarian sector has always helped me to appreciate working in the ED. After a day of pushing humanitarian issues or creating a strategy for the MGB system, it is so important to take the time to experience the ED and to see patients. I’ve always felt it as a privilege to live in both worlds — to move between large global systems and being a doctor taking care of patients at the bedside. It’s a wonderful gift to be able to do both.